
Since the description of the axillary approach to the brachial plexus block by Dr Halstead et al. in 1884, it has become the most performed peripheral nerve block for forearm and hand surgery, mainly due to the low incidence of complications and increased patient satisfaction [1–3]. Using ultrasound (USG) for brachial plexus block has become the standard of care. USG-guided axillary plexus block is a technically feasible, safe and effective modality that allows visualisation of the individual nerves. Better visualisation ensures minimum tissue trauma, decreased incidence of nerve damage, and the use of lower doses of local anaesthetic, hence reducing complications [4]. The median, ulnar and radial nerves are arranged around the axillary artery but may be subject to anatomical variation. The musculocutaneous nerve may be located between the biceps and coracobrachialis muscle, within the coracobrachialis muscle or near the median nerve [1, 5–8]. Identifying the individual nerves and separate blockade of the four main constituent nerves significantly increases the success rate [3, 4]. Despite prevalent use of USG to perform peripheral nerve blocks, most anaesthesia providers still position the extremity as per landmark-oriented approaches that were generally based on anatomical studies. For example, the brachial plexus in the axil-lary region is approached with the extremity positioned as Winnie [9] described with the shoulder and elbow at 90º [4]. The brachial plexus at the axillary level is also susceptible to rearrangement of its structures according to the arm’s position [4]. Hence, in this study, we decided to find the optimum arm position to visualise the brachial plexus at the axil-la using USG. The primary objective was to study USG visibility of the brachial plexus at the axilla in three different arm positions commonly used for block performance. The secondary objective was to correlate the visibility with age, gender, body mass index (BMI), and laterality.
METHODS
This prospective observational study was conducted in 36 adults of either sex above 18 years of age posted for upper limb surgery from June 2021 to December 2023 at a tertiary care hospital after institutional ethics committee approval (vide approval number ECR/266/Lokmanya/Inst/MH/ 2013RR-16-REF NO: D02021080 dated 7 May 2021). Written informed consent was obtained for participation in the study and use of the patient data for research and educational purposes. The research was conducted following the principles of the Declaration of Helsinki, 2013. Those refusing to participate, with shoulder movement restrictions, BMI greater than 35 kg m–2, local swelling, pain, and infection, were excluded from the study. USG examinations were performed by senior experienced anaesthesio-logists using one USG machine (Samsung Sonoace R7) with a linear multifrequency probe of 5–12 MHz. The probe was placed perpendicular to the nerves, artery and humerus (short axis) at the intersection between the lower border of the pectoralis major muscle and the biceps brachii muscle. Probe pressure exerted on the skin was just enough to cause light compression of veins. Each arm was placed in three different positions using a goniometer:
1) shoulder at 90º and elbow at 90º (90/90) (conventional);
2) shoulder at 90º and elbow at 0º (90/0);
3) shoulder at 120º and elbow at 90º (120/90).
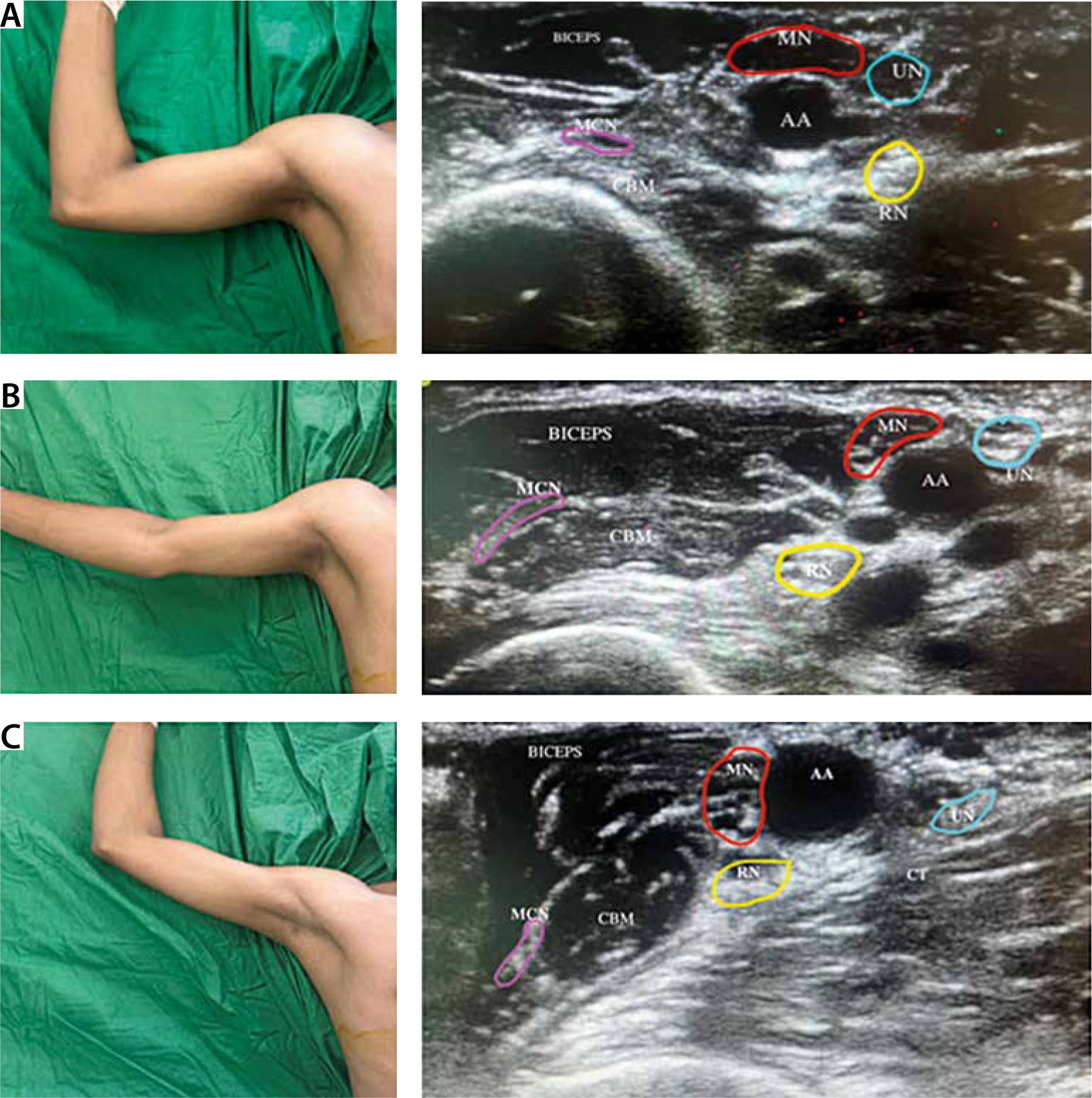
Images were captured, saved, and encrypted during each scan for subsequent viewing and assessment. In each scan radial, median, ulnar and musculocutaneous nerves were assessed for visibility using a six-point visibility scale: 0 – no nerve identified, 1 – nerve identified with a high probability, 2 – nerve identified, but most of it not visible, 3– nerve identified, more than 50% of its borders can be precisely distinguished from surrounding structures, 4 – nerve completely visible, but fascicles poorly defined, 5 – nerve completely visible and multiple fascicles identifiable [4, 10]. The USG probe was then moved slowly down from the axilla to the elbow joint, following the path of each nerve and then back to the axilla for confirmation of the nerve [5]. Thereafter, skin to the axillary artery and skin to the individual nerve (median, ulnar, radial and musculocutaneous) distances were measured in centimetres (cm). Also, the distance between each nerve and an axillary artery was noted in cm (Figure 1). For subjects in whom the musculocutaneous nerve could not be seen, scanning was performed 5 cm below the previous point (point of intersection of pectoralis major muscle and biceps brachii). The need to scan downward was noted.
RESULTS
A sample size of 36 patients per group was derived from previous literature, with 90% statistical power, 5% level of type I error (a) and 10% type II error (b). The means were compared using the t-test or ANOVA test, as appropriate. All tests were three-tailed, and differences with a P-value ≤ 0.05 were deemed statistically significant. The correlation of BMI, gender and laterality with visibility score was calculated using Pearson’s correlation coefficient. The data was analysed using the IBM SPSS Statistics application, version 25.
The mean age of our study population was 33.80 ± 11.91 years, with 80.6% of the population being male. The average BMI was 24.57 ± 3.91 kg m–2: 52.8% of the study population had average body weight, eleven patients (30.6%) were overweight, four patients (11.1%) were obese, and 2 (5.6%) patients were underweight [3].
We studied the left hand in 22 (61.1%), whereas the right hand was studied in 14 (38.9%) of the study sample.
Skin-axillary artery (S-AA), skin-median nerve (S-MN), skin-ulnar nerve (S-UN), skin-radial nerve (S-RN) and skin-musculocutaneous nerve (S-MCN) distances were shortest in arm position 120/90 and longest in arm position 90/90. However, the diffe-rence was not significant (Table 1, Figure 2).
TABLE 1
Summaary of parameters in three different arm positions
[i] S-AA – skin to axillary artery, S-MN – skin to median nerve, S-UN – skin to ulnar nerve, S-MCN – skin to musculocutaneous nerve, S-RN – skin to radial nerve, AA-MN – axillary artery to median nerve, AA-UN – axillary artery to ulnar nerve, AA-MCN – axillary artery to musculocutaneous nerve, AA-RN – axillary artery to radial nerve.
FIGURE 2
A) Comparison of distance from skin to nerves in 3 arm positions. B) Comparison of distance from axillary artery to nerves in 3 arm positions
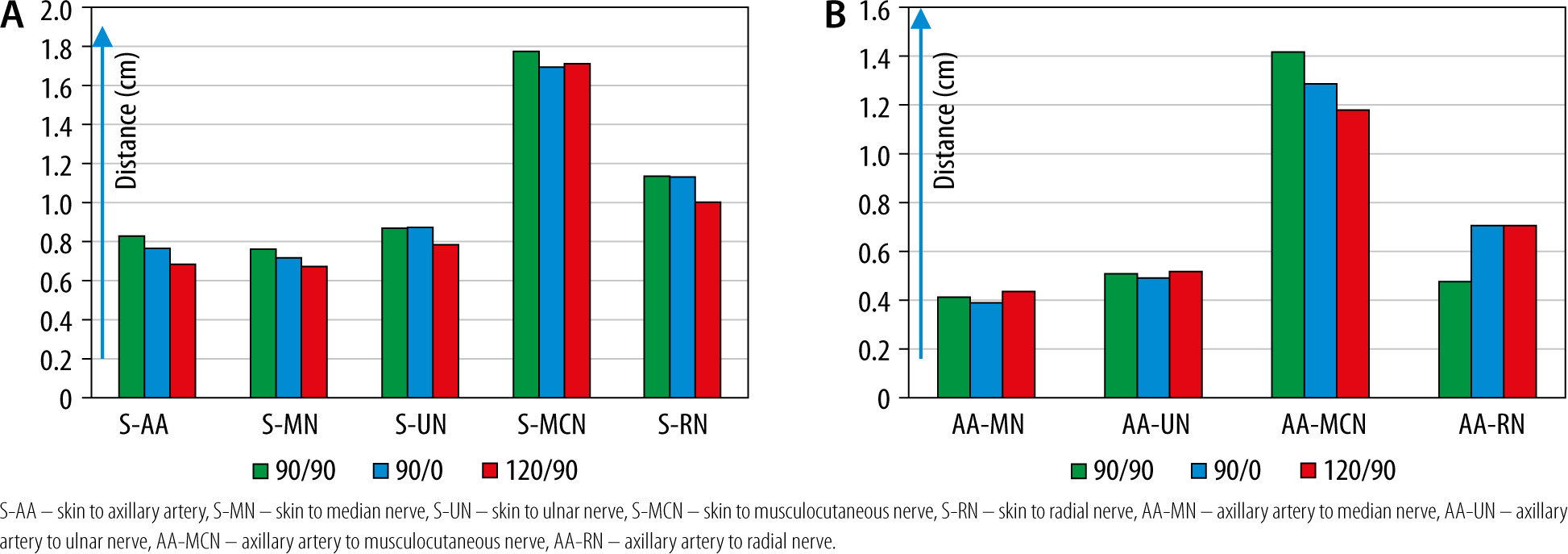
Axillary artery-nerve distances were comparable in all positions (Table 1, Figure 2).
It was necessary to scan downwards to visualise the musculocutaneous nerve in 2 patients in position 90/90, 1 patient in position 90/0 and 3 patients in position 120/90.
The visibility scores for individual nerves and the mean visibility scores were comparable in all three groups (Table 1, Figure 3).
FIGURE 3
Mean visibility score of median nerve (MN), ulnar nerve (UN), musculocutaneous nerve (MCN), radial nerve (RN)
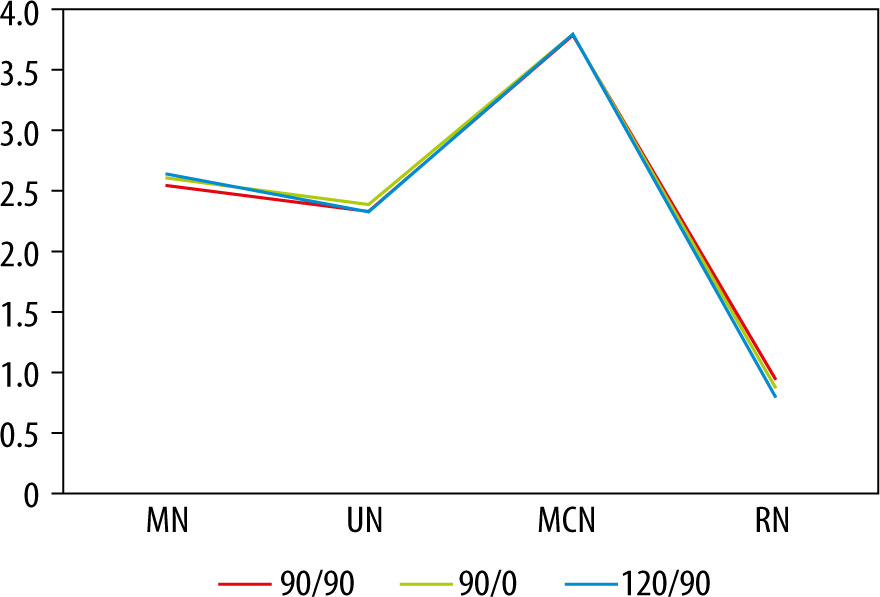
The radial nerve could not be visualised in 25% of patients in the 90/90 position, 30% in the 90/0 position and 19% in the 120/90 position, but this was not statistically significant (P = 0.55).
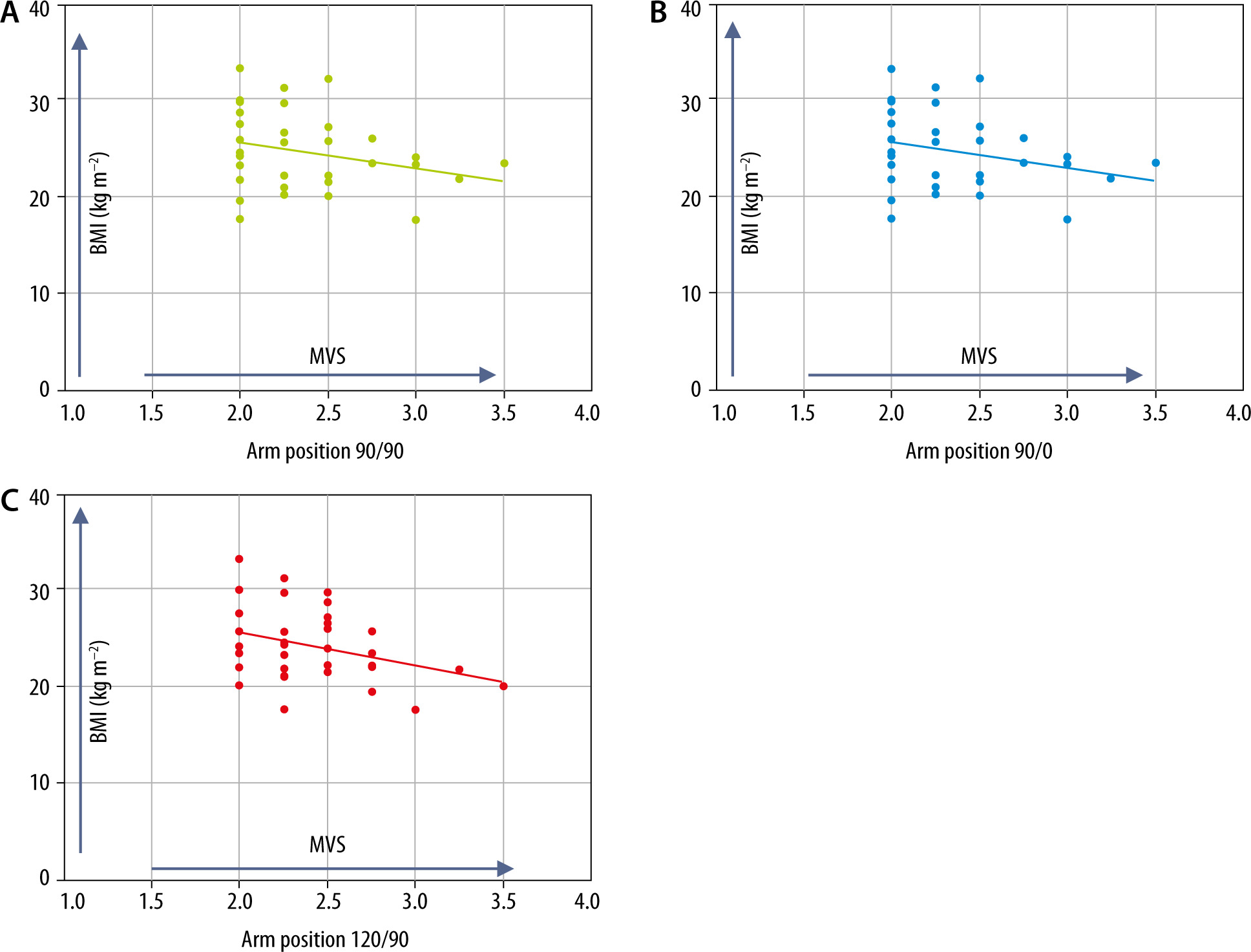
There was a negative correlation between BMI and the mean visibility score in all three positions, but it was comparable in all three groups (Figure 4). Similarly, the correlation of laterality and gender with mean visibility scores was comparable.
DISCUSSION
Various researchers have described the individual nerves and their morphology at the axilla on USG [1, 7, 11–13]. Individual nerves’ scanning and tracing techniques for their precise localisation have also been delineated [5, 14, 15]. The frequent anatomical variations and rearrangement of the nerves in the axilla after various degrees of arm abduction emphasise the need to locate individual nerves [16–20] separately. Even with the advent of USG, extremities are often positioned as if performing landmark-oriented approaches with the shoulder and elbow at 90 degrees [3, 9]. However, there is a dearth of literature describing other positions. Demographic data in our study was comparable to previous studies [3, 4, 6, 8, 12]. Various authors scanned and labelled the intersection junction between the lower border of the pectoralis major muscle and the biceps brachii muscle as the proximal position (P) and a point 5 cm distal to this as position ‘D’. They noted findings in both locations in all the patients [3, 4, 6]. We decided to scan the axilla in the distal location only if the musculocutaneous nerve was not visualised in location P. In our study, it was necessary to scan downwards in 2, 1 and 3 patients in 90/90, 90/0 and 120/90 groups, respectively.
The S-AA and the skin-nerve distances were the shortest in 120/90 position and the longest in position 90/90. This was comparable to observations of previous researchers who studied the distances in the infraclavicular region [16, 17]. However, another researcher had variable results [4]. A possible explanation for this would be that stretching the muscles and tissues with increasing arm abduction causes a decrease in their cross-section thereby making the nerve more superficial and accessible [4, 8, 16, 17]. This could minimise the tissue trauma while approaching the nerve.
The artery-nerve distances were comparable in different arm positions, as in the findings of previous researchers [4]. Other researchers favoured the 160–180 shoulder position for the AA-MCN distance [8].
Ozturk et al. [3] measured the median nerve–musculocutaneous nerve distance, which was shortest in the 90/0/D position, and considered it safer and more effective for axillary nerve block. They did so because the musculocutaneous nerve lies outside the neurovascular bundle and is subject to frequent anatomical variations. It is also vital to block it for complete forearm anaesthesia.
Our study showed that the visibility of the nerves was similar in all three positions. In contrast, a previous researcher found significantly higher visibility scores in the shoulder 180 positions for all nerves [4, 16, 17]. However, using the 180° shoulder position is highly unlikely in routine practice as it can cause pain, discomfort and excessive stretching of tissues and nerves.
The radial nerve could be visualised more often in 120/90, but this was not statistically significant. However, Wong et al. [12] (90/0 position) could locate the radial nerve in 95% of their scans, with poor visibility in 30%. Their success in finding the radial nerve was attributed to combined use of USG and nerve stimulation, allowing more precise localisation. The difficulty in imaging the radial nerve may be because of its depth and tendency to lie in the shadow of other structures, such as the axillary artery, the axillary veins and the ulnar nerve, compared with the more superficial nerves. The angle of the radial nerve path relative to the skin surface may exacerbate the difficulty.
The musculocutaneous nerve had the best overall visibility in all three positions (3.77 ± 0.50). We could identify the musculocutaneous nerve in all patients compared to some previous researchers [3].
Our study found a negative correlation between BMI and mean visibility, whereas some researchers found no correlation between the two [3].
In conclusion, the nerve artery distances and visibility were comparable in all three arm positions. So, our primary objective was not reached. The skin-artery and the skin-nerve distances were shortest in the 120/90 positions; also, the radial nerve could more often be seen in this position. Though these results were not statistically significant, they could be clinically important.
The limitation of our study was that we did not examine the efficacy of the block performed. Further studies will be needed to compare the efficacy of the block in these three arm positions.