
Dear Editor,
Patients with pre-existing pulmonary conditions are at increased risk of severe COVID infection [1]. These patients have limited physiologic reserve to compensate, making them more susceptible to experiencing hypercapnic and/or hypoxic respiratory failure with COVID pneumonia [1]. Pulmonary alveolar proteinosis (PAP) is one such entity, marked by copious production of surfactant proteins that obstruct gas exchange in the alveolar membrane [2]. With severe hypoxic respiratory failure, treatment involves supportive therapy of supplemental oxygen and clearance of secretions, including whole lung lavage. Here we present a case of whole lung lavage to treat hypoxic respiratory failure due to PAP flare in the setting of COVID pneumonia.
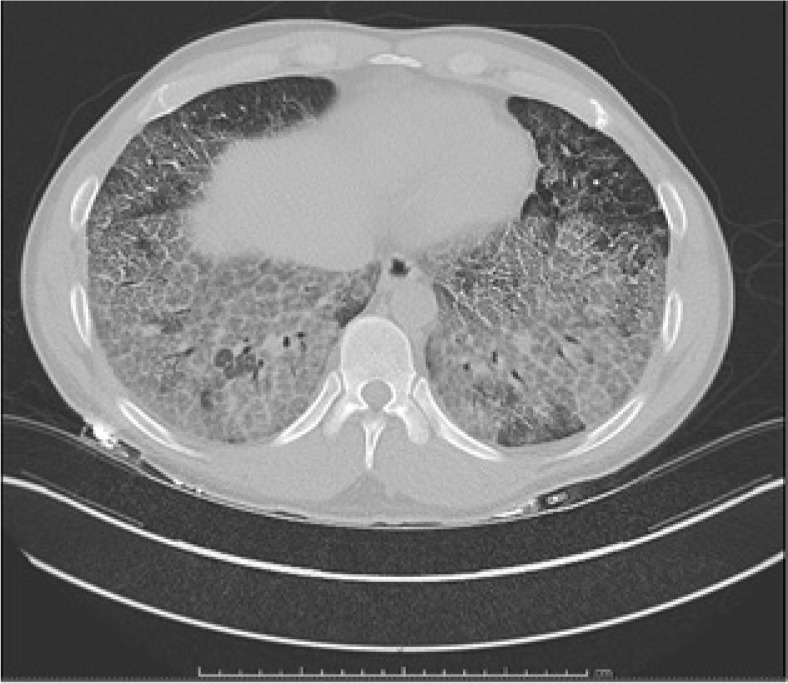
The patient was a 30-year-old man with a history of PAP previously treated with granulocyte-macrophage colony- stimulating factor (GM-CSF) and whole lung lavage, who presented to the hospital with shortness of breath and cough. Upon evaluation, he was found to be positive for COVID-19 infection with subsequent COVID pneumonia. His chest computed tomography showed diffuse ground-glass opacities with crazy paving, which was consistent with a flare of his underlying PAP (Figure 1). He was admitted to the me-dical intensive care unit, where he was treated with antibiotics and dexame-thasone, with only mild improvement in his respiratory status.
FIGURE 1
Computed tomography of the chest without contrast study revealing ground-glass opacities with crazy paving consistent with pulmonary alveolar proteinosis
The patient continued to have respiratory distress, requiring oxygen supplementation with a high-flow nasal cannula. He was periodically placed in the prone position to maintain his oxygenation with pulse oximetry above 90%. On transthoracic echocardiogram (TTE), the patient also had evidence of pulmonary hypertension and mild right heart dysfunction. A multi-disciplinary discussion was conducted with the intensive care team and pulmonology, cardiothora-cic surgery, and anesthesiology specialists. A decision was made to proceed with whole lung lavage under general anesthesia with veno-arterial extracorporeal membrane oxygena-tion (VA-ECMO) on standby. VA-ECMO was preferred over veno-venous extra-corporeal membrane oxygenation given the evidence of mild right heart dysfunction on TTE. Cardiothoracic surgery would be readily available for peripheral arterial and venous cannulations if ECMO was required.
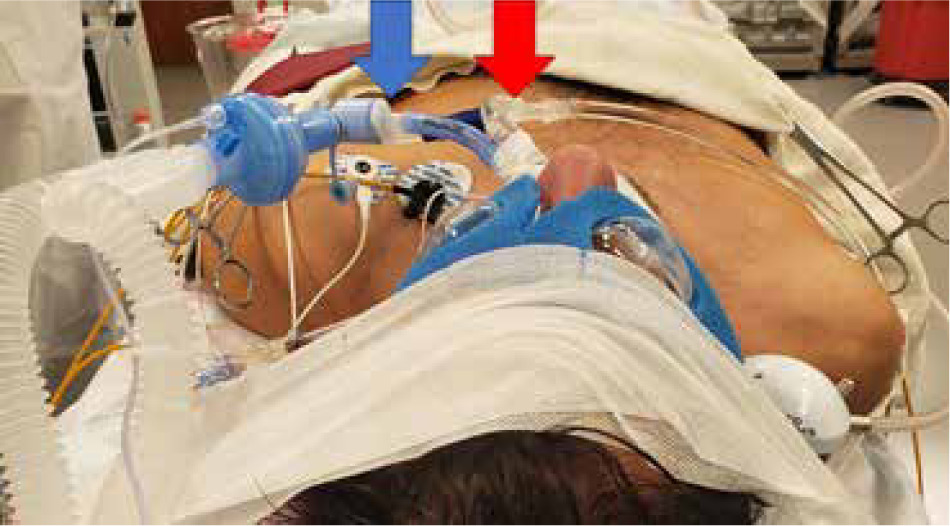
General anesthesia was administered, and a left-sided double lumen tube was placed (Figure 2). Arterial and venous cannulation was performed. The left lung was isolated and vented, allowing for maximal decompression. Whole lung lavage was performed with instilled 500 mL aliquots. With each aliquot, chest percussion was performed, followed by drainage of the lavage fluid. In total, 16 L of fluid were instilled and drained (Figure 3). The drained fluid was mixed with bleach, given the patient’s COVID-positive status. At the end of the procedure, the double lumen tube was exchanged for a single lumen tube, and the patient returned to the operating room the next day for the same procedure on the right lung. This stepwise approach was taken to allow for adequate pulmonary recovery before proceeding with whole lung lavage of the contralateral side.
FIGURE 2
Left-sided double lumen tube utilized to ventilate one lung (blue arrow) while being able to lavage the contralateral side (red arrow)

During the procedure, the patient experienced transient episodes of desaturation. In response to significant desaturation, the lavage was paused, and the patient was given recruitment maneuvers with manual ventilation until saturations improved to levels above 85%. Additionally, arterial blood gases were drawn hourly to confirm adequate oxygenation, ventilation, and acid-base status. Bronchoscopy was also performed to ensure that no lavage fluid was entering the ventilated lung.
After both lungs had been treated by lavage, the patient recovered in the Intensive Care Unit. The next day, he was extubated and placed on 2 L of oxygen via a nasal cannula. He was subsequently discharged on home oxygen and inhaled sargramostim (a glycosylated recombinant human GM-CSF) for maintenance of his PAP.
Our patient with both COVID pneumonia and PAP flare presented a unique challenge in maintaining oxygenation. Here we discuss the key factors that impair gas exchange: PAP, COVID pneumonia, and whole lung lavage during one-lung ventilation.
PULMONARY ALVEOLAR PROTEINOSIS
PAP has various etiologies, with autoimmune being the most common [2]. Others include congenital or secondary to another disease that results in excessive protein [2]. Regardless of the etiology, all cases lead to increased surfactant production, increased effective alveolar membrane thickness, and impaired gas exchange. While supportive therapies are helpful, the standard treatment is whole lung lavage, wherein large volume saline is introduced into the airways, percussion of the chest is utilized to free the proteinaceous material into suspension, and the whole slurry is evacuated [3]. This process is repeated until the saline runs clear, which often requires multiple rounds of lavage. Bronchoscopy can be performed to visually assess the clearance of secretions. Following whole lung lavage, immunomodulation therapy, such as GM-CSF, can be administered to assist in neutrophil clearance of the excess alveolar surfactant [4]. Close follow-up must be conducted to assess the need for supportive therapies or further lavage.
CONSIDERATIONS WITH ACTIVE COVID PNEUMONIA
COVID can significantly impact patients during the pathogenesis of PAP and during whole lung lavage. Firstly, COVID has the potential to further impair the ability of the alveolar membrane to perform gas exchange, by causing inflammation and increased thickness of the membrane [2]. Supportive therapies may include supplemental oxygen, non-invasive positive pressure ventilation, intubation with mechanical ventilation, and ECMO [2]. Additionally, COVID can complicate the patient’s ability to tolerate whole lung lavage. With the fluid-filled lung temporarily unavailable to perform any gas exchange, ventilating the non-operative lung may be challenging in COVID patients, potentially requiring implementation of more aggressive, invasive therapies such as ECMO to maintain oxygenation. Finally, COVID presents an infectious hazard to the proceduralist performing the whole lung lavage due to repeated bronchoscopy and airway manipulation [2].
ANESTHETIC CONSIDERATIONS OF WHOLE LUNG LAVAGE
Anesthetic management begins with preoperative optimization. The patient’s oxygen requirement, ventilatory function, and functional capacity can provide an indication of how well the patient would tolerate one lung ventilation. In cases of mild COVID infections, the anesthesiologist may consider delaying the procedure until the infection has resolved. However, in severe infections, where whole lung lavage could greatly improve the patient’s gas exchange, the benefits of the procedure may outweigh the risk of intraoperative hypoxia.
Intraoperatively, it is imperative to maintain adequate oxygenation and ventilation [3]. Strategies to mitigate ventilation-perfusion mismatch during lavage include performing the lavage on one lung at a time and lateral decubitus positioning. Additionally, the proceduralist can take breaks from lavage and the anesthesiologist can perform recruitment maneuvers with 100% inspired oxygen on the ventilated lung [5]. ECMO can also be considered if the patient is persistently hypoxic despite employing the above strategies.
Postoperatively, the patient may experience pulmonary edema from the lavage. Appropriate supportive therapies, diuretics, and close monitoring can be implemented to optimize recovery. A PAP flare in the setting of acute COVID pneumonia presents a particular challenge to the anesthesiologist during treatment with whole lung lavage. Excess surfactant, hyper-inflammatory state, and lavage all impair gas exchange at the alveolar membrane, inhibiting adequate oxygenation and ventilation. Effective management involves frequent assessment of these parameters with intraoperative monitoring and preparation for ECMO if less invasive measures fail.
CONCLUSIONS
This case reflects the challenges of treating PAP in a patient with concomitant acute COVID infection. There are many anesthetic considerations of both whole lung lavage and active COVID pneumonia that need to be considered for patient and provider safety. A multi-disciplinary team approach and careful preoperative planning is imperative for successful treatment.