
Bacteraemia in critically ill patients carries a risk of significant morbidity and mortality – a risk that is higher if the infecting organism is multidrug-resistant (MRO) [1]. Apart from increased mortality, it is asso-ciated with longer hospital length of stay, higher costs and repeated hospitalisations [2, 3]. There is genuine concern that despite advances in healthcare and dia-gnostic facilities, the prevalence of MRO infections in the intensive care unit (ICU) population is rising [4, 5].
Colonisation or infection with MROs has significant implications for critically ill patients. There are implications for infection control and prevention and the choice of appropriate empirical antibiotic therapy for this group of patients [6]. On the other hand, inappropriate use of antibiotics against MROs is asso-ciated with significant risks, such as the development of drug-resistant organisms, the selection of drug- resistant organisms and adverse effects from these antibiotics. This raises the critical question of whether we can quantify the risk posed by colonisation and subsequent bacteraemia by the same organism, as this will have broader implications for the possible choice of empiric antibiotics in this group, MRO surveillance and infection control and prevention practices.
Various risk factors have been identified for colonisation with MROs. Factors such as recent and prolonged hospitalisation, ICU stay, residency in a long-term care facility, high severity of illness, immunosuppression, indwelling catheters and gut mucosal barrier injury are some factors that have been demonstrated to predispose to colonisation with MROs [7, 8]. Almost all these risk factors are present in the ICU population, putting them at increased risk of acquisition of colonisation with MROs. MROs such as vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant Gram-negative bacteria (MDR-GNB) colonise the gastrointestinal and respiratory mucosa in critically ill patients. In conditions such as shock, multi-organ failure or following chemotherapy and/or radiotherapy, the mucosal barrier is breached, causing mucosal barrier injury [9, 10]. This may result in bloodstream infections (BSIs) secondary to the colonisation. Several studies have identified colonisation as a significant risk factor for subsequent bacteraemia with Acinetobacter baumannii [11].
However, only a limited number of studies have examined the broad relationship between colonisation by MROs and subsequent bacteraemia [12–19]. Most have studied patients in a non-ICU setting, and at least two have been underpowered due to a small sample size [12–16, 18]. These studies predominantly included a cohort of patients with haema-tological and oncological malignancy [12, 15].
Given the limitations of extrapolation of these data onto the critically ill, we thought of conducting a study in our ICU, a large tertiary ICU admitting various subgroups of patients, including patients with major trauma, neurosurgical conditions and general medical and surgical conditions. We aimed to determine the prevalence of colonisation, the risk of MRO bacteraemia associated with colonisation and the risk of mortality related to MRO bacterae-mia. Given the results of the above studies, we hypothesised that colonisation with MROs predisposes to BSIs with the same organism.
METHODS
Study setting
The study was conducted at Westmead Hospital, a 700-bed tertiary care teaching hospital in the Western metropolitan region of Sydney. The level III ICU is a 36-bed mixed medical-surgical unit that manages critically ill medical, surgical, trauma, and neurosurgical patients. The ICU admits approximately 1,300 patients per annum and has a bed occupancy of approximately 90–95%.
Patients are admitted to the ICU either electively or following emergency surgery from the operating theatre. Alternately, acutely unwell patients are admitted from the emergency department, hospital wards, or close observation units.
Study design
This was a single-centre retrospective cohort study of patients admitted to the ICU between 1 January 2014 and 31 March 2019. The Western Sydney LHD Human Research Ethics Committee (2019/ETH/12568) reviewed and approved the study proposal, waiving participants’ consent.
MRO surveillance
All patients undergo a routine surveillance swab within 24 hours of admission to check for colonisation by multidrug-resistant organisms. Swabs collected from the anterior nares and perineal region are processed in the laboratory for MRSA, VRE and MDR-GNB. The MRSA assay was a PCR assay on the BD Max platform (Staph SR) done directly from the sample. The VRE assay was a PCR assay developed in-house and done directly from the sample on a BD Max platform. The MDR-GNB swabs were first cultured on a Muller-Hinton agar plate with ampicillin, and subsequently, directed PCRs were carried out on the BD Max platform.
As part of the ICU infection control policy swabs were done on admission, discharge and twice weekly on Mondays and Thursdays.
Inclusion and exclusion criteria
All patients (≥ 18 years of age) admitted to the ICU between January 1, 2014, and March 31, 2019, were included. Patients with features of brain death at the time of admission or imminent demise were excluded. Brain death was determined using the criteria of the Australia and New Zealand Intensive Care Society (ANZICS).
Data collection
Three searchable patient databases were accessed for this study, and data were merged using the medical record number (MRN), patient name, and patient date of birth as identifiers. The ICU adult patient database and the electronic medical records (eMR) were searched for surveillance swabs and blood culture results for the study period. The ICU adult patient database is a database into which data are entered prospectively on patient admission to the ICU. This database provided patient-related information on all admissions to the Westmead ICU during the study period. This included data on demographics, date, time and source of admission, type and principal reason for ICU admission, APACHE (Acute Physiology and Chronic Health Evaluation) score, details of ICU interventions, ICU outcome, and ICU and hospital length of stay.
The other two databases were the surveillance swab and blood culture databases. These data were extracted from the eMR using the ICU as the patient’s location at the time of collection of swabs and blood cultures. Patients with more than one ICU admission during the same hospitalisation were identified, and surveillance data from the multiple ICU admissions were merged under the same hospital admission. The surveillance swab and blood culture results (from the eMR) were matched to the individual records in the ICU adult patient database using the MRN identifier. Blood culture collection was at the discretion of the treating clinician. Results of multiple cultures from a patient during the same hospitalisation were recorded chronologically alongside the surveillance data to enumerate the number of patients who had a positive MRO blood culture.
Missing or incomplete data
The analysis did not include data on patients with missing or incomplete records.
Terms and definitions
Colonisation was a positive surveillance result. Bloodstream infection due to an organism was defined as recovery of the organism from at least one blood culture. A multidrug-resistant organism was an MRSA, VRE or MDR-GNB (extended spectrum β-lactamase producing Enterobacterales [ESBLE] and carbapenemase-producing Enterobacterales).
The screening swab results of all patients were reviewed for the isolation of MRSA, VRE or MDR-GNB in blood culture. For this study, isolation of an organism in blood culture drawn at least 48 hours after a swab report showing a similar organism was taken as having developed a BSI with the same organism. This chronological sequence was necessary to demonstrate that the positive swab having preceded the BSI may have predisposed to the BSI.
Study objectives
The study’s primary objectives were to determine the prevalence of colonisation with MROs and quantify the risk of bacteraemia associated with MRO colonisation. A secondary objective was to assess the mortality risk related to MRO bacteraemia.
Statistical analysis
Continuous data were presented as mean and standard deviation (SD) for normally distributed variables, median and interquartile range (IQR) for non-normally distributed variables and frequency (n) and percentage (%) for categorical variables. Where data were found to be normally distributed, Student’s t-test was applied. The c2 or Fisher’s exact test was used to assess the significance of the association of categorical or nominal data. All tests were two-sided, and a = 0.05 was accepted as the significance level.
Risk was estimated as odds, and the odds ratio was calculated from the formula as follows:
Both crude and adjusted odds ratio estimates were calculated. Binary logistic regression analysis was used to adjust for confounders, and the adjusted risk estimates were presented as odds ratios (OR) with 95% confidence intervals (CI). All analyses were carried out using SPSS Version 21.0 (Armonk, NY: IBM Corp).
RESULTS
Study population
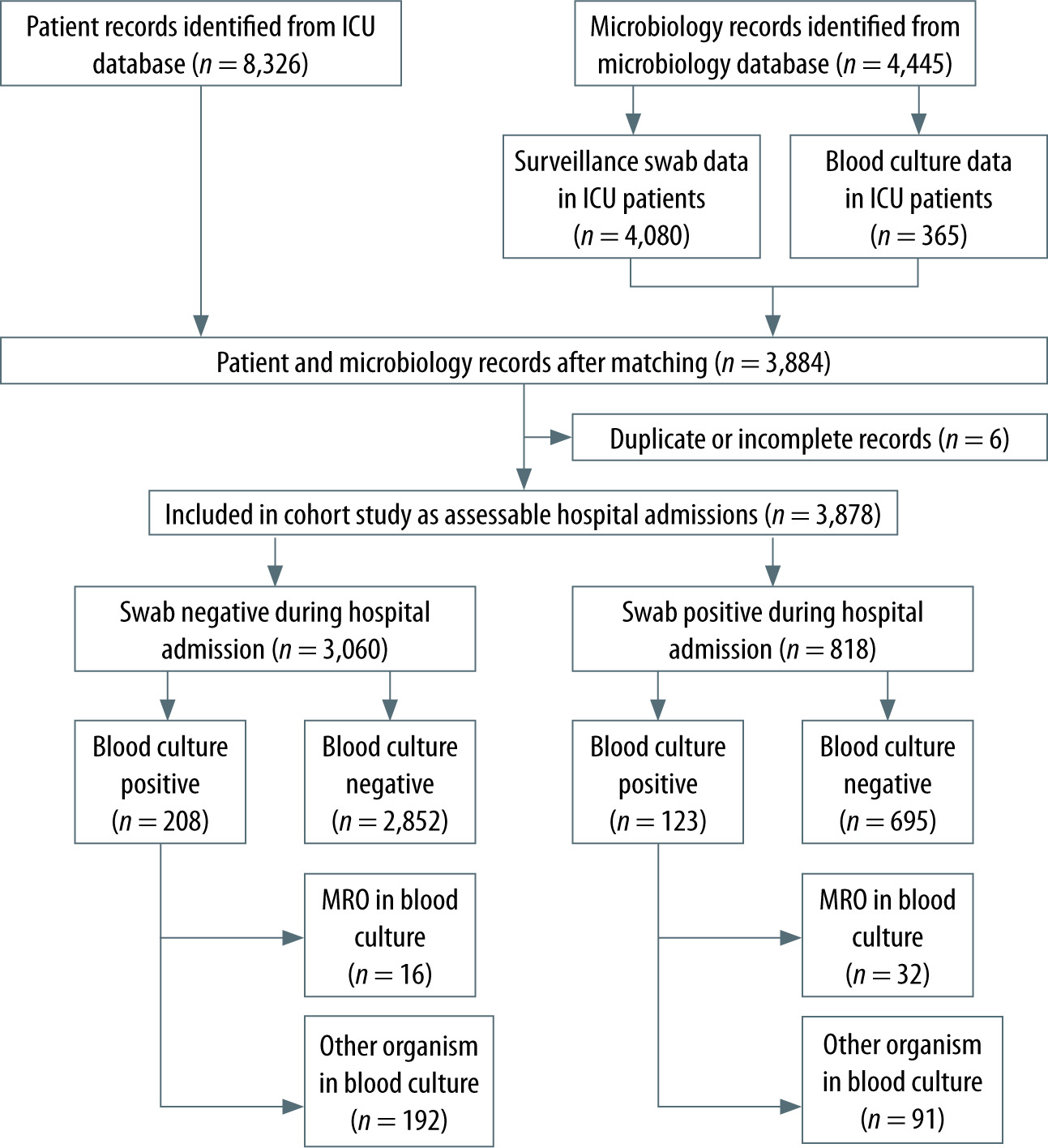
There were 3,878 assessable patients among 8,326 ICU patient records over the study period. Six (0.07%) patient records were duplicate entries, and an additional 555 (6.6%) patient records were related to ICU readmission of patients during the same hospitalisation. As we planned to study each hospitalisation episode, we merged the data of the first ICU admission and subsequent ICU admissions. |Of the remaining 7,765 patient records, 347 (4.1%) could not be matched, and a further 3,887 (46.6%) did not have any swab data either because the patient’s admission was short (< 24 h) or because swabs were not obtained (Figure 1).
Patient characteristics
The mean age of the study cohort was 58 years (SD 18). Most of these patients were male (61.5% male, 38.5% female). The median APACHE-II score was 17 (IQR 12.0–22.0). There was a preponderance of medical admissions (60.9%) compared to surgical admissions (39.1%), reflecting the overall admission pattern in the ICU. Most admissions to the ICU were between 8:00 am and 4:00 pm (64.8%) and not after hours, and these came predominantly from the OT (1,465/3,878 = 37.7%) or ED (1,039/3,878 = 26.7%). Sepsis with or without shock was the leading APACHE-II diagnosis (333/3,878 = 8.5%) among the study cohort (Tables 1 and 2).
TABLE 1
Study cohort
TABLE 2
Patient and ICU admission characteristics at baseline
MRO swab results
Of all patients in the study, 818 (21%) were swab positive for MROs, and the remaining 3,060 (78.9%) were swab negative. The overall prevalence of MRO colonisation in our cohort was 21%.
9,681 swabs were obtained from 3,878 patients (median of two swabs per patient). Of these, 6,764 were negative for MROs (69.8%), and 2,917 were positive in their surveillance swabs. Amongst patients whose admission swabs returned a negative result, a higher proportion had ≤ 2 swabs done per admission, compared to those whose swabs returned a positive outcome: 2,206 (72%) vs. 396 (48.4%). Thus, a higher proportion of admissions who turned out positive in their surveillance swabs had > two swabs per episode compared to the swab negatives (51.6% vs. 27.9% respectively), possibly reflecting a longer ICU length of stay.
Among the swab positives, 272 (33.6%) were posi-tive for VRE, 235 (28.7%) were positive for MDR-GNB, and 166 (20.3%) were positive for MRSA (Table 3). In addition, 121 (14.8%) were positive for two of three organisms, and 24 (2.9%) were positive for all three organisms. Almost as many patients were swab positive after ICU admission (≥ 48 hours after the first ICU admission) as were positive at admission to the ICU.
TABLE 3
Baseline swab data related to patients enrolled in study cohort
Bloodstream infections
There was a higher proportion of positive blood cultures among the swab positive patients than the swab negative patients (15% vs. 6.8%). The number of blood cultures positive for MROs (3.9% vs. 0.52%; P < 0.001) or positive for other organisms 11.1% vs. 6.2%; P < 0.001) was significantly higher in the swab positive group compared to the swab nega-tives (Table 4). Significantly, swab positives were associated with a higher proportion of patients with positive blood cultures with MROs than the swab negatives (3.9% vs. 0.52%) (Table 4). The mortality was significantly higher among the swab positives than negative patients (20.7% vs. 13.1%; P < 0.001). However, this difference was not observed among those positive for MROs (1.2% vs. 0.2%; P = 0.67) on blood culture or those positive for other organisms (2% vs. 1.2%; P = 0.91) on blood culture compared to those negative on blood culture.
TABLE 4
Outcome of swab positive (colonised) and swab negative (non-colonised) patients
Risk of adverse outcome
The overall risk of BSI (including MROs and other organisms) was significantly higher amongst swab positive patients compared to those who were swab negative (15% vs. 6.8%; P < 0.001). BSI with MROs was considerably higher in the swab positive group compared to the swab negative group (Table 5). The odds ratio for BSIs in the swab positive group compared to the swab negative group, adjusted for acuity of illness and length of stay, was 6.3 (95% CI: 3.40–11.76). Likewise, the risk of bacteraemia due to organisms other than MROs among swab positive patients was also significantly higher (adj. OR 1.37 (95% CI: 1.04–1.82)).
TABLE 5
Risk of bloodstream infection and mortality among patients colonised with MROs
The risk of mortality among swab positive patients who were MRO positive on blood culture was similar to mortality risk among swab negatives who were MRO positive on blood cultures (adj. OR 0.91 (95% CI: 0.09–19.50)) (Table 5). The hospital length of stay was longer in the swab positive group than in the swab negatives (Table 4).
DISCUSSION
This study demonstrated an increased risk of BSI with MROs in patients colonised with the same organism compared to non-colonised patients. The adjusted odds ratio for BSIs with MROs was 6.3 (95% CI: 3.40–11.76). Our study showed a statistically significant increase in all-cause mortality in the swab positive group compared to the swab negative group. However, when subgroups of MRO bacteraemia or non-MRO bacteraemia patients were compared, no significant difference in mortality was observed. Like our observations, Vehreschild et al. [16] found an increased association of ESBLE BSI with previous colonisation (OR 52; 95% CI: 5.71–473.89). Liss et al. [17] reported a risk ratio for developing ESBLE BSI of 4.5 (95% CI: 2.89–7.04) and a risk ratio for the development of VRE bacteraemia of 10.2 (95% CI: 7.87–13.32). Both these studies examined a cohort of haematological/oncological malignancy patients in a predominantly ward setting but did not report on mortality among bacteraemic patients [16, 17]. Our study did not find an increase in mortality associated with bacteraemia, whether in the swab positive or negative groups. This is in keeping with the results from other studies [15]. That notwithstanding, overall all-cause mortality was higher in the swab positive group. This may be ascribed to the increased severity of illness noted in this group of patients. On the other hand, it is possible that the sample size was too small to detect a small but significant difference in mortality when considering only patients with MRO bacteraemia.
Another important finding was that our cohort’s overall prevalence rate of MRO colonisation was 21%, with VRE being the most prevalent organism. While 50.7% were positive for MROs on surveillance swabs at admission to the ICU, 48.8% turned positive 48 hours after their admission to the ICU, most likely because of colonisation occurring in the ICU. Studies have reported a colonisation rate between 3 and 29%, but the prevalence rate may vary from unit to unit and cohort to cohort [4, 15, 17].
The high prevalence of MRO colonisation (> 20%) noted in our study has implications for infection control and prevention. The Infection Prevention and Control Practice Handbook published by the New South Wales (NSW) Government’s Healthcare Associated Infection Program recommends single-room isolation and/or cohorting such patients. Surveillance for MROs is recommended at admission to the ICU and regular intervals for all patients [20]. The results of this study also have implications in terms of the choice of empirical antibiotics in the treatment of patients colonised with MROs. A few studies in the past have examined this relationship between the appropriateness of the selection of empirical antibiotics in this group of patients and outcomes. They have demonstrated increased mortality associated with inadequate empirical antibiotic cover in critically ill patients who are colonised with MROs [8, 21]. Given the above and the results of this study, one could make a case to start appropriate empirical antibiotics in that group of patients who are colonised, have had a protracted course in the hospital, have a high severity of illness or have other risk factors associated with MRO colonisation and bacteraemia. Our study also noted that approximately 50% of patients returned positive surveillance swab results after admission to the ICU after having tested negative on admission. This may be the subject of further audits/investigations into implementing local infection control and prevention policies.
This is the only study investigating the relationship between MRO colonisation and bacteraemia with the same organism in a general ICU population admitting multiple groups of patients. This study is also one of the most extensive, looking at 3,878 hospitalisation episodes and 9,681 surveillance swab results. This is also the only study that has examined the three main groups of MROs in the same study population: VRE, MRSA and MDR-GNB. Kanagasingham et al. [19] studied the sensitivity and specificity of MRSA and methicillin-sensitive Staphylococcus aureus (MSSA) PCR assays in predicting concurrent or subsequent infections in a similar population. They demonstrated that the assays have high specificity and a negative predictive value in predicting MRSA and MSSA infections.
The main limitation of our study was that it was a single-centre observational study. Therefore, it can only establish association and not causation. Secondly, the data used were prospectively collected and maintained in the ICU database, and other data were extracted from the electronic data records. These data were largely non-validated. Human error during data entry could affect subsequent data analysis and interpretation, which remains a challenge in utilising and analysing such data. The number of swabs taken for patients was variable. This is undoubtedly an important source of bias. Although information was available, we did not precisely control the number of swabs taken for each patient. As a surrogate, we controlled for the duration of stay in the final analysis. A median number of swabs taken (and IQR) for the two groups is provided. We did not specifically study the characteristics or differences between patients with more and those with fewer swabs. Lastly, we only included patients admitted to the ICU in our analysis. Therefore, our results may not be generalisable to non-ICU patients.
CONCLUSIONS
This study demonstrates an association between MRO colonisation and subsequent BSI among critically ill patients in a mixed medical-surgical ICU. This finding has broader implications for infection control and prevention measures and perhaps for choosing empirical antibiotics to treat a select group of colonised patients.