
Dear Editor,
Hip fracture in older adults is one of the most frequent occurrences in orthopedic surgery. There is now ample evidence that mortality is increased if surgery is delayed beyond 48 hours [1].
It is common for these patients to use anticoagulant or antiplatelet drugs whose withdrawal time is sometimes insufficient to perform spinal anesthesia (SA).
Numerous papers describe the use of peripheral nerve blocks in patients undergoing surgery for femur fracture, but only in terms of perioperative analgesic efficacy [2].
However, in the literature there are no reports of patients with femur fracture undergoing internal fixation under peripheral nerve blocks only.
In our center, patients undergoing surgery for proximal femur fracture who are taking antiplatelet or anticoagulant therapy, whose withdrawal time is not compatible with the performance of SA, routinely receive surgery under locoregional anesthesia and sedation.
We describe a case of an 85-year-old patient with pertrochanteric hip fracture.
Her medical history includes: obesity (body mass index: 51), chronic obstructive pulmonary disease on O2 therapy, previous myocardial infarction on clopidogrel therapy, and previous postoperative delirium following ge-neral anesthesia (GA) a few years earlier. She has been classified as American Society of Anesthesiologists (ASA) physical status/risk category III.
The patient signed informed consent to perform the surgery under peripheral locoregional anesthesia and sedation.
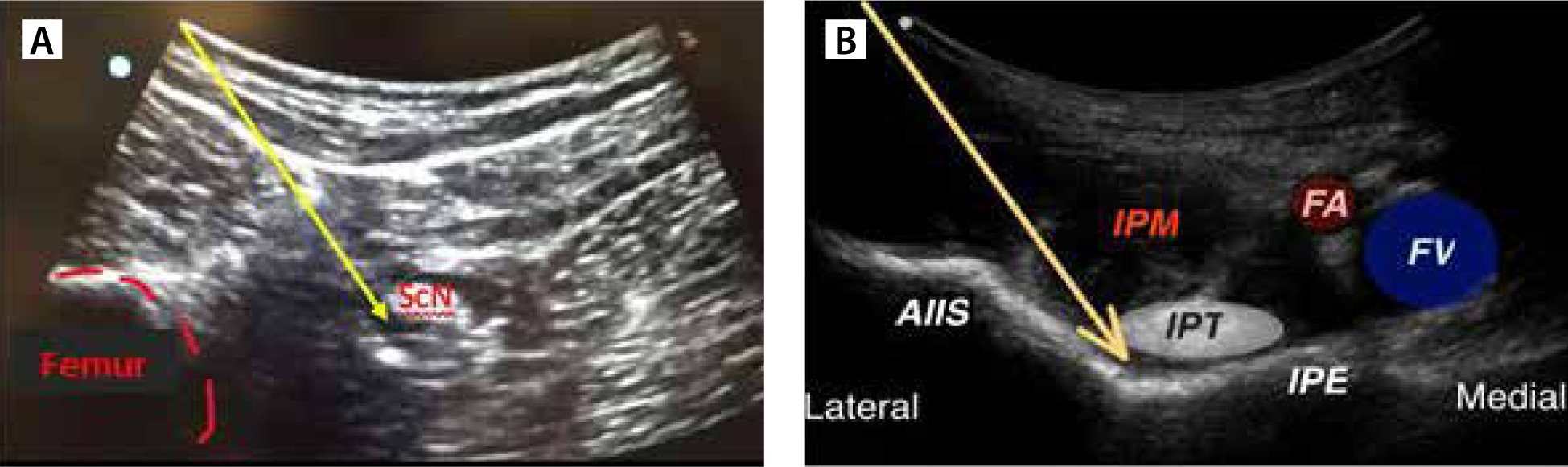
We prepared a 1 : 1 mixture of 2% mepivacaine and 0.5% ropivacaine and performed locoregional anesthesia with ultrasound-guided technique as follows (Figure 1):
FIGURE 1
A) Anterior sciatic nerve block. B) PENG block via a lateromedial approach: local anesthetic was placed in the plane between the iliopsoas tendon (IPT) and iliopubic eminence (IPE). AIIS – anterior inferior iliac spine, FA – femoral artery, FV – femoral vein, IPM – iliopsoas muscle, ScN – sciatic nerve
We combined intraoperative sedation with remifentanil.
Vital parameters were monitored and remained stable throughout the surgery, which lasted 70 min.
The patient experienced no pain at the surgical incision, and no other sedative or analgesic drugs had to be added during the surgery.
In the postoperative period, standard analgesic therapy was set with paracetamol 1 g every 8 h and the patient did not receive additional analgesics.
Surgery for hip fracture is performed in most cases under SA and, where not possible, under GA [6]. Peri-pheral nerve blocks are almost always used to control postoperative pain.
In our center, in these cases, surgery is routinely conducted under peripheral locoregional anesthesia, because peripheral nerve blocks can be performed in patients on anticoagulation or antiplatelet therapy, where SA is contraindicated.
Anterior sciatic nerve block is considered a deep block by European guidelines and as such would have the same contraindications as SA in terms of antiplatelet drugs [7].
However, it is now proven that the ultrasound-guided approach, with real-time visualization of the needle tip and perineural injection, results in very low tissue trauma with a very low incidence of hematoma. Moreover, spinal hematoma would be a much more serious eventuality.
In conclusion, we believe that locoregional anesthesia is a valid alternative to GA in frail patients undergoing femur fracture surgery in which SA is contraindicated.
It could also serve as a basis for performing randomized trials to compare locoregional anesthesia with SA or GA in terms of postoperative mortality and morbidity and length of hospitalization.