

Dear Editor,
Opioid-based intravenous patient- controlled analgesia (iv-PCA) is primarily used for postoperative pain management in spinal surgery in which instruments are inserted into the vertebral body, such as in vertebral fusion surgery. This is because of concerns regarding the risk of surgical site infection (SSI) when foreign bodies such as epidural catheters are inserted near the instrumentation. There are no conceivable postoperative pain management strategies other than iv-PCA with opioids, leaving the patient with inadequate pain management and a risk of unpredictable opioid-related side effects. Therefore, anaesthesiologists are always interested in more effective regional anaesthesia strategies, including neuraxial analgesia such as epidural or spinal analgesia, to reduce the side effects of systemic opioid administration.
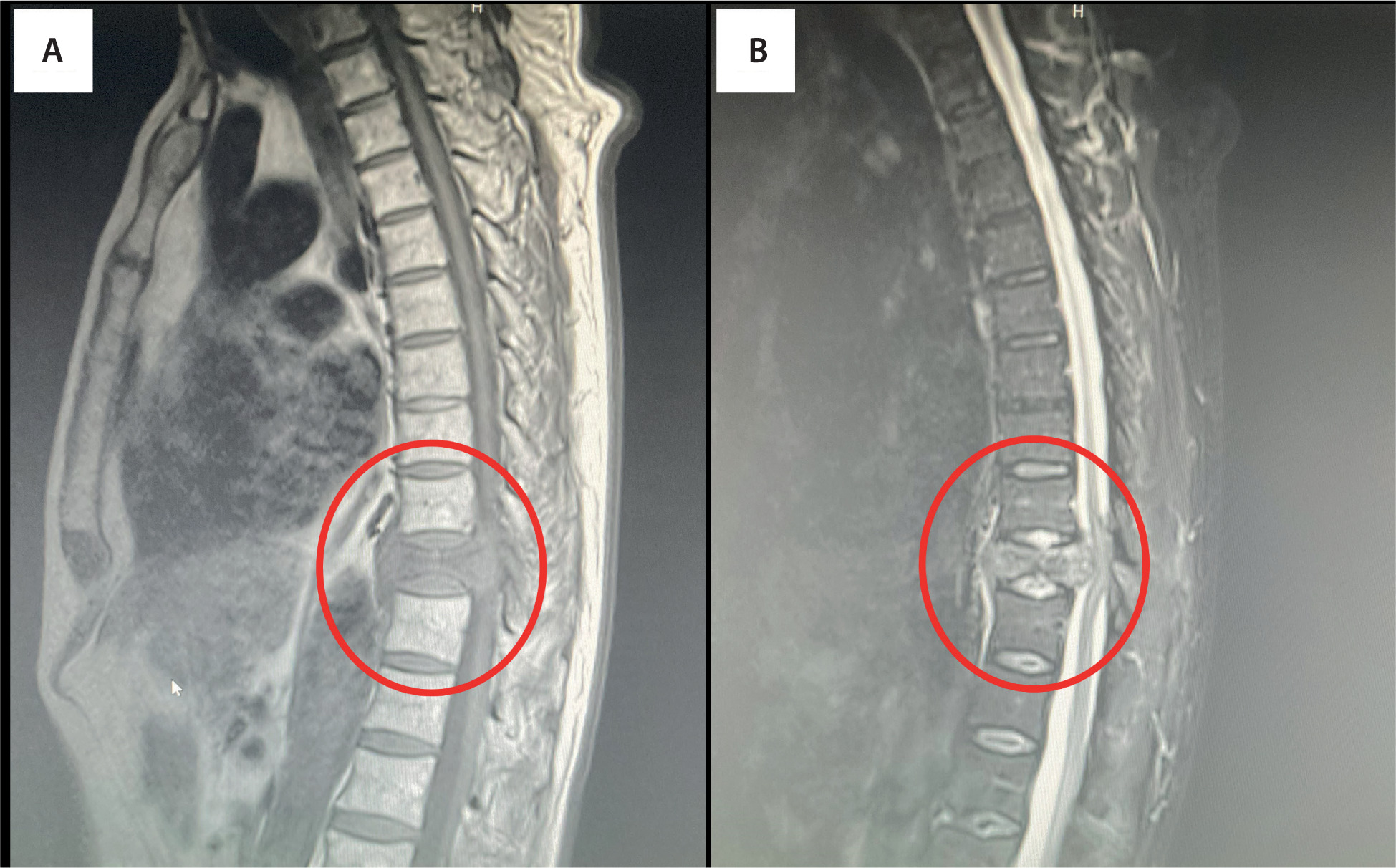
The patient described in this letter was a 73-year-old man (height, 172 cm; weight, 67 kg) with back pain as the chief complaint. His medical history included treatment for hypertension, hyperlipidaemia, and urolithiasis. Six months previously, he had experienced back pain after shovelling snow, but it had resolved spontaneously. However, two weeks prior to admission, the back pain reappeared and worsened gradually. The following week he became aware of numbness in both soles of his feet and had difficulty walking. He consequently visited a local orthopaedic surgeon, and a compression fracture of the 10th tho- racic vertebra was identified on computed tomography. He was referred to our orthopaedic department and admitted for close examination and treatment. On examination at admission, slight paraesthesia in both flanks, of which he was unaware, was noted. Magnetic resonance imaging (Figure 1) revealed a suspected pathological fracture of the 10th thoracic vertebra due to the metastasis of an unknown primary cancer. His clinical symptoms were confirmed to be consistent with a pathological compression fracture of the 10th thoracic vertebra. Posterior spinal fusion surgery of the 8th–12th thoracic vertebrae and resection of the 9th–10th thoracic vertebral arches were scheduled for pain relief and spinal cord decompression.
FIGURE 1
Magnetic resonance imaging showing a suspected pathological fracture of the 10th thoracic vertebra. Magnetic resonance imaging revealed a suspected pathological fracture of the 10th thoracic vertebra, owing to the metastasis of an unknown primary cancer; it showed a low signal on T1-weighted imaging (A) and a high signal on short inversion time inversion recovery imaging (B) of the 10th thoracic vertebra
Vertebral surgery with instrumentation is associated with severe postoperative pain. In addition, surgery at multiple vertebral levels causes even more severe postoperative pain. Inadequate postoperative analgesia and opioid-related adverse effects are therefore of even greater risk in situations where there is a considerable increase in intravenous administration of opioids. We often experience cases where iv-PCA with opioids alone does not provide sufficient postoperative analgesia, but increasing its dose is also challenging because patients experience unpredictable opioid-related adverse effects such as nausea or dizziness. In a previous study, the postoperative pain in the patient-controlled epidural analgesia (PCEA) group, administered using an epidural catheter inserted by an orthopaedic surgeon under direct vision at the end of surgery, was significantly lower and achieved significantly higher mobilization capacity than the iv-PCA group after spinal surgery for spondylodiscitis [1]. Given these circumstances, epidural analgesia seemed to be the most promising strategy for postoperative pain management in our patient. How ever, he had unperceived bilateral slight flank paraesthesia and numbness in both soles of the feet. The use of local anaesthetics for epidural analgesia was questionable, especially when postope rative neurological findings needed to be evaluated. Therefore, epidural analgesia using morphine alone, without local anaesthetics, was considered the most suitable postoperative pain management in this case. Because hydrophilic morphine administered into the epidural space would diffuse to the intrathecal space and exert its analgesic effects in a broad dermatome to the head through cerebrospinal fluid circulation [2, 3], the epidural catheter could be inserted at the lower lumbar level, well away from the surgical site. Intraoperative analgesia was planned primarily with remifentanil owing to the slower onset of neuraxial morphine.
An epidural catheter was inserted 5 cm into the epidural space at L5/S1 before the induction of general anaesthesia. While the patient was preoxygenated, 2 mg of morphine and 5 mL of saline were mixed and administered via the epidural catheter. After a bolus administration of 6 mg of remimazolam to induce anaesthesia, continuous administration of 0.2 μg kg–1 min–1 of remifentanil and 0.8 mg kg–1 h–1 of remimazolam was initiated. After intubation and positioning of the patient in the prone position, surgery was initiated (47 min after the administration of 2 mg of morphine). Remifentanil administration was maintained in the range of 0.2–0.4 μg kg–1 min–1, while remimazolam was administered continuously at 0.7–0.8 mg kg–1 h–1 until the completion of surgery. Bispectral index values were consulted as a reference. The balloon system of the epidural catheter was filled with 8 mg of morphine and 300 mL of saline (approximately 0.0027%), and continuous administration of morphine was initiated at 4 mL h–1 (approximately 0.11 mg h–1) 43 min after the start of surgery (90 min after the initial morphine administration). The surgery duration was 149 min. On completion of the surgery, remimazolam was discontinued, and remifentanil was reduced to 0.1 μg kg–1 min–1. After postoperative radio graphy was conducted in the prone position and the patient was placed in the supine position, remifentanil was discontinued. After the administration of flumazenil (0.5 mg), the patient was quickly awakened and extubated. The time from the initial morphine administration to extubation was 220 min. The patient complained of no pain other than pulling discomfort in the back, which was assumed to be due to the new alignment of the erector spinae muscles, caused by the posterior spinal fusion surgery and instrumentation. After confirming that his respiratory status and consciousness level were normal, the patient was transferred from the operating room to the orthopaedic ward without pain, 79 min after the completion of surgery (275 min after the initial morphine administration). The patient was managed using the same postoperative monitoring of SpO2, electrocardiography, and blood pressure as patients undergoing epidural postoperative pain management with local anaesthetics mixed with morphine. Acetaminophen combined with other non-steroidal anti-inflammatory drugs was additionally administered when necessary for postoperative pain management. The postoperative pain score was 0 at rest and < 2 during body movement on the visual analogue scale from the night of surgery. The balloon system of the epidural catheter was emptied, and the continuous administration of morphine was concluded on the third postoperative day. The epidural catheter was removed after it was confirmed that the pain had not increased. A very high satisfaction level was obtained not only from the patient, but also from the ward nurses who provided his postoperative care.
Successful postoperative pain management is an important factor for enhanced recovery after surgery; it leads to improvements in clinical outcomes and cost savings for patients [4]. Failure in postoperative pain management is a risk factor for postoperative delirium (POD) [5], and POD is associated with worse patient outcomes, including mortality, in fields such as cardiac [6], non-cardiac [7], and spinal surgery [8]. A multicentre study of postoperative pain on the first postoperative day following 179 common surgical procedures including abdominal surgery, orthopaedics, and otolaryngology reported that postoperative pain after spinal fusion surgery ranks high [9]. One meta-analysis reported that PCEA was more effective than iv-PCA for pain management after spinal fusion surgery [10]. The effect of morphine administered to the epidural space at the thoracic level and that at the lumbar level are comparable in blunt chest trauma in terms of pain management, incidence of pulmonary complications, and occurrence of morphine-related side effects [11]. Taking these considerations and the patient’s neurological symptoms into account and to resolve the concern of SSI, the epidural catheter was inserted at a low lumbar level (L5/S1), and morphine was administered alone into the epidural catheter without local anaesthetics. However, at extubation, 220 min after the initial morphine administration to the epidural catheter, it had already taken analgesic effect, so the patient did not complain of pain or show changes in neurological symptoms.
The continuous administration was set at 4 mL h–1 using a balloon system in the current case, only because we used the equipment available at our hospital. However, the dose (mg h–1), not the rate (mL h–1), of continuous administration of morphine was the critical factor, because the aim of admi nistering hydrophilic morphine to the epidural catheter was to provide it to the intrathecal space as well, that is, the diffusion of hydrophilic morphine to the intrathecal space.
Intrathecal and epidural administration of opioids for pain management after spinal surgery has already been reported to be effective, as mentioned above [10, 12, 13], and may not be a new approach to postoperative analgesia in spinal surgery. However, the neuraxial administration of opioids alone without local anaesthetic for pain management after spinal surgery in patients who already pre sent with neurological symptoms, as in the present case, is unique and a promising idea to ensure better patient satisfaction with postoperative analgesia than with the administration of opioid iv-PCA.
This letter suggests that epidural anaesthesia using only opioids without local anaesthetics could be a promising and effective postoperative pain management strategy for surgery where severe postoperative pain is a concern, but epidural anaesthesia is often avoided, such as spinal surgery with instrumentation. Good postoperative pain control was successfully achieved using an epidural catheter inserted at the lower lumbar spine level, well away from the surgical site, during posterior spinal fusion surgery of multiple vertebrae at the thoracic level, in the current patient with neurological symptoms.
This strategy of epidural administration of hydrophilic morphine alone without local anaesthetics could also be applied in scoliosis surgery with a long surgical site or severe Cobb angle, in which there are concerns of new neurological symptoms developing after correction, but with severe postoperative pain that is difficult to manage.
Written informed consent for publication was obtained from the patient.