
Dear Editor,
Cerebral vasculitis is a rare compli- cation of pneumococcal meningitis, associated with high mortality and a substantial incidence of persistent neurological sequelae [1–5]. There is no standardized treatment for this cerebrovascular complication; how- ever, it is evident that intervention should address not only the infectious trigger but also the complex under- lying inflammatory cascade [1, 3]. Pro- phylactic corticosteroid therapy with dexamethasone, administered within the initial four days alongside antibio- tic therapy, has been shown to reduce mortality and the incidence of deaf- ness [4]. Nevertheless, there is a lack of necessary evidence to recommend corticosteroid therapy as a treatment within established post-infectious vasculitis [1, 5]. Additionally, there is no evidence regarding the use of immunosuppressants or apheresis in these cases [5]. Many specialists tend to adopt therapeutic regimens estab- lished for systemic or primary cerebral vasculitis [2].
A 29-year-old man with a history of childhood traumatic brain injury with post-traumatic cerebrospinal fluid fistula presented with a two-day history of headache before he was found at home with a low level of con- sciousness (Glasgow Coma Scale, GCS < 7). Orotracheal intubation was perform ed, and he was transferred to the referral hospital, where a plain comput ed tomography (CT) scan re- vealed a generalized reduction in the depth of sulci and fissures. The CT angiogram did not show any patho- logical findings. In the laboratory tests, there was an elevation in acute phase reactants (procalcitonin on admission of 40 ng mL–1), and a fever of up to 39ºC was noted during the examina- tion. A chest X-ray without infiltrates, normal urine sediment, and cultures were obtained. A lumbar puncture was performed, yielding turbid fluid with biochemical evidence of bacte- rial meningitis. Treatment was initiated with dexamethasone and empiric tri- ple antibiotic therapy. Subsequently, sensitive pneumococcus was cultured from the cerebrospinal fluid and from blood, prompting a switch to targeted treatment with cefotaxime. Despite being kept without sedation, the pa- tient maintained a GCS score of 4 with pathologic extension of upper limbs in response to pain. He retained corneal and cough reflexes but lacked a threat reflex.
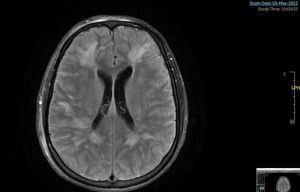
Given the poor clinical progres- sion, a lumbar puncture was repeat- ed at 72 hours, revealing aseptic fluid, and a follow-up CT scan was conduct ed, revealing multiple areas of hypodensity in subcortical and periventricular white matter with bi- lateral and symmetric involvement of semioval centres. A subsequent magnetic resonance imaging (MRI) scan (Figure 1) demonstrated multiple confluent focal areas of restricted dif- fusion bilaterally and symmetrically, predominantly in the frontal and bi- lateral periatrial regions, as well as in the semioval centres, consistent with cytotoxic damage, suggesting acute ischaemic lesions in the con- text of probable associated vasculitis.
FIGURE 1
Initial magnetic resonance imaging: multiple confluent focal areas of restricted diffusion bilaterally and symmetrically, predominantly in the frontal and bilateral periatrial regions, and in the semioval centres, consistent with cytotoxic damage, suggesting acute ischaemic lesions in the context of probable associated vasculitis. Bilateral frontal punctate susceptibility artefacts, within the signal alteration, suggestive of small haemorrhagic foci
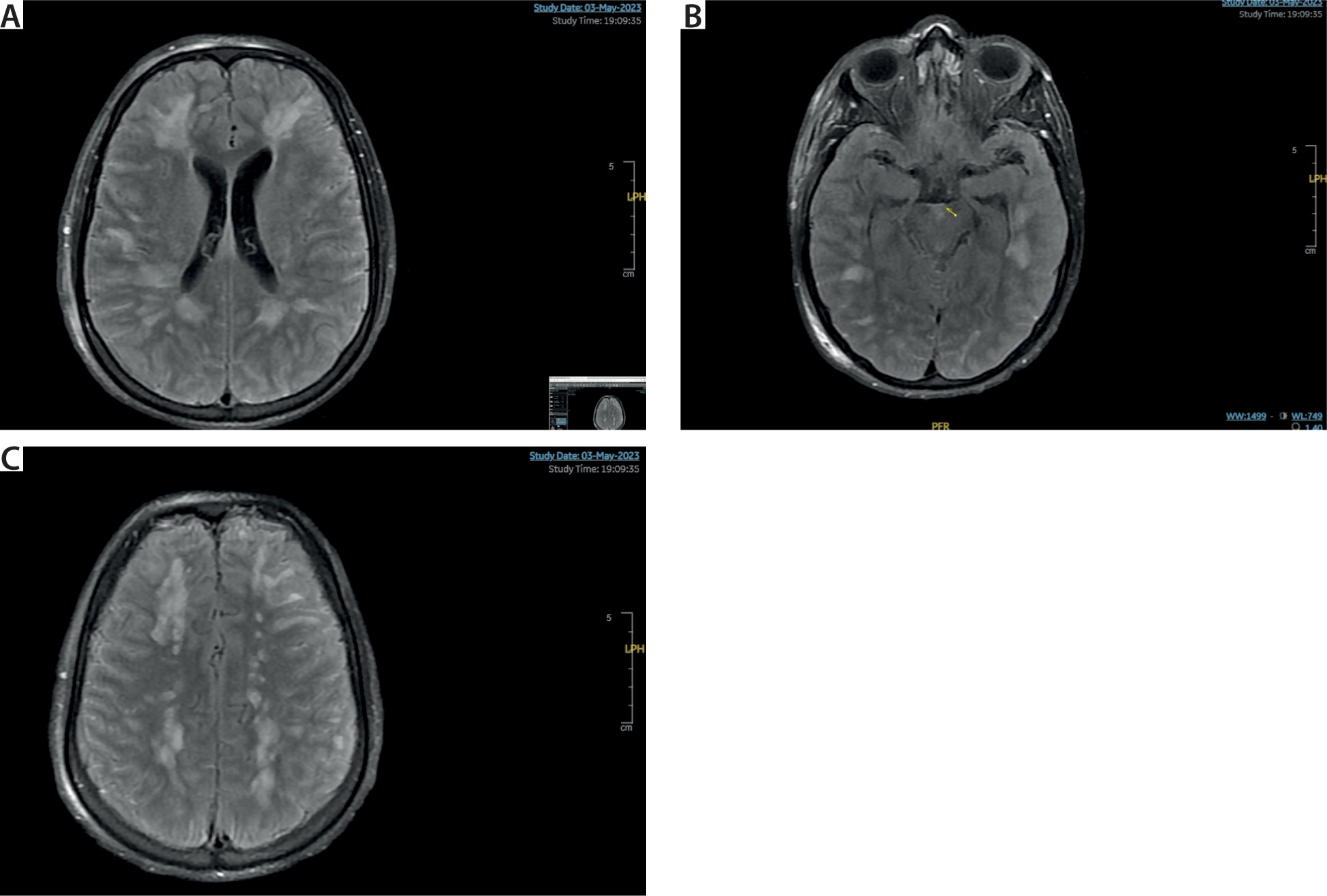
Additionally, bilateral frontal punctate susceptibility artefacts were observed within the signal alteration, sugges- tive of small haemorrhagic foci. A 3D time-of-flight vascular study showed normal morphology of the major ves- sels of the Willis polygon. No signs of cerebral venous thrombosis were noted. Leptomeningeal enhancement was observed in the context of menin- gitis. Cerebral angiography and biopsy were not performed.
An extension study was conduct- ed, including a transthoracic echocar- diogram and chest-abdomen-pelvis CT, to rule out embolic causes and vasculitis at other levels. The microbio- logical investigation was expanded, along with a comprehensive rheuma- tological analysis, all yielding negative results. Multiple electroencephalo- grams (EEGs) were conducted to rule out non-convulsive status epilepticus as the cause of coma.
The patient was diagnosed with post-infectious cerebral vasculitis due to pneumococcus, and treatment com - menced with pulses of 1 g of me thyl- prednisolone for 5 consecutive days, followed by 60 mg per day. By the 7th
day, neurological evolution remained unfavourable, resembling the presen- tation upon admission. Subsequently, plasmapheresis was initiated after rul- ing out sepsis. A total of 10 cycles were performed with albumin replacement, with a volume of 3000 mL of replaced plasma in each session, spacing them every other day after the 5th session.
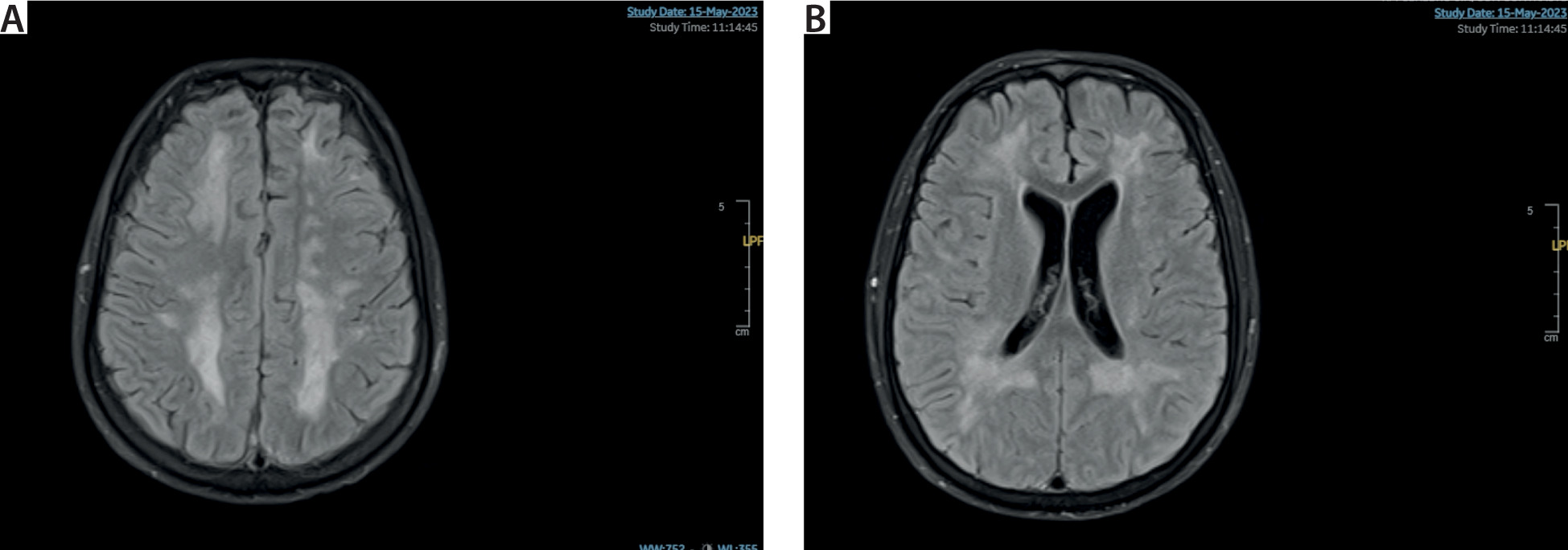
MRI was repeated on the 16th day of admission (Figure 2). Changes in sig- nal characteristics were described on this imaging study. Most previously de- scribed lesions tended to confluence and increased in size on conventional sequences with normalization in diffu- sion sequences. Within the described lesions, punctate areas of higher signal intensity were observed in diffusion sequences with clear apparent diffu- sion coefficient restriction. Following intravenous contrast administration, multiple areas of intraparenchymal enhancement were observed, cor- responding to previously described areas of diffusion restriction, without pathological leptomeningeal enhan- cement. New areas of paraventricular haemorrhagic content adjacent to the right lateral ventricle were noted, with undetermined clinical relevance. In- creased visualization of sulci, fissures, and the ventricular system was noted. The findings were interpreted as evo- lution to chronicity of previously de- scribed lesions.
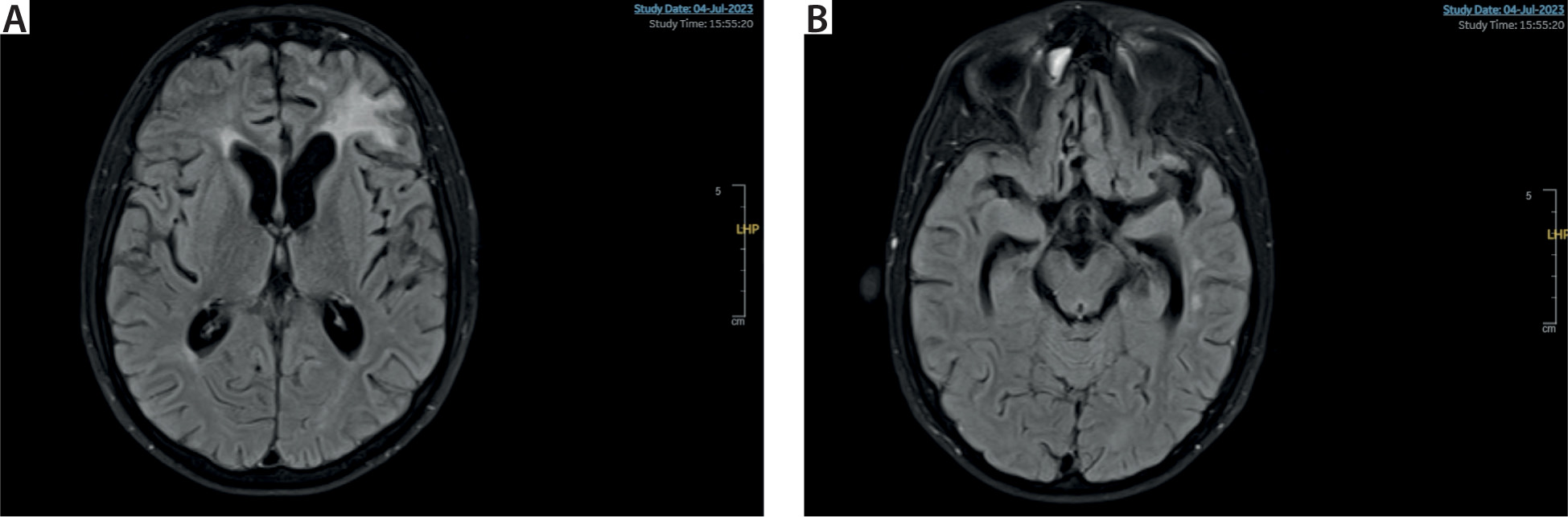
Progressively, the patient showed improvement in neurological exami- nation, and successive control EEGs demonstrated resolution of encepha- lopathy. At the time of discharge from the Intensive Care Unit, 36 days after admission, the patient was conscious, partially oriented, followed simple commands, and exhi bited coherent language. After two months of hospi- talization, repeat MRI (Figure 3) showed radiological improvement in the de- scribed lesions and stability of haemor- rhagic lesions. Increased visualization of sulci, fissures, and the ventricular system was noted.
Upon discharge from the hospi- tal one month later, the patient was able to walk with assistance and was independent in basic activities of daily living, although there were neurocog- nitive deficits. At present, the patient is fully independent. However, mild cog- nitive impairment persists. Consent for publication of this case report was given by his legal guardians.
The pathophysiology of post- infectious cerebral vasculitis is poorly understood [6, 10]. It is postulated that following the initial treatment with bactericidal antibiotics, pneumococ- cal death and lysis occur, leading to the massive release of bacterial com- ponents and activation of the inflam- matory cascade [10]. This process results in disruption of the blood-brain barrier, recruitment of leukocytes through the endothelium, and cellular damage [6]. However, many researchers believe that the pathophysiology could be more complex and might vary depending on the implicated pathogen [10]. Never- theless, immune system activation fol- lowing bacterial lysis in some cases gives rise to the development of cere- bral vasculitis [10]. Biopsy confirmation, although the gold standard diagnostic method, is rarely performed [10].
Treatment aims to eradicate the in- fectious agent while also addressing the inflammatory cascade [6]. Only dexamethasone has demonstrated clinical efficacy as an adjuvant therapy alongside antibiotic treatment during the early days of the disease [8]. How- ever, the impact of corticosteroids on ischaemic brain injury secondary to vasculitis is unknown [6]. Several iso- lated clinical cases suggesting their effectiveness have been published, including some describing clinical re- lapse after de-escalation or discontin- uation of treatment [9]. Nevertheless, there is no evidence supporting their use, and even less literature support- ing the administration of immunosup- pressants or plasmapheresis in this context [6]. In fact, based on the lite- rature search conducted, we did not find other clinical cases with a similar therapeutic approach.
We are uncertain whether the clinical improvement in our patient was due to prolonged corticosteroid use, therapeutic apheresis, or the natural course of the disease [6]. In the case of plasmapheresis being a valid thera- peutic resource, it is unknown wheth- er the effect could be attributed to the removal of an unknown circulating antibody or to the anti-inflammatory effect of plasmapheresis itself [6].
Our case suggests that plasma- pheresis therapy could be beneficial for late complications of pneumococ- cal meningitis associated with vascular inflammation.